






procedure / elbow Arthroplasty of the Elbow: Partial or Total Elbow Protheses
Arthroplasty of the Elbow: Partial or Total Elbow Protheses

Primary idiopathic osteoarthritis or post-traumatic arthritis, rheumatoid arthritis or ankylosing spondylarthritis, sus and intercondylian region fractures of the elbow in the elderly and fracture of the radial head, as well as other conditions (tumors, hemophilia…) benefit from total elbow replacement by arthroplasty.
Description :
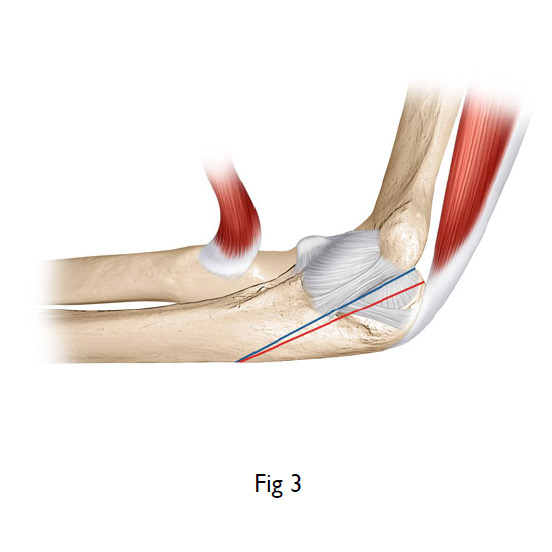
The elbow is a joint connecting the lower extremity of the humerus (trochlea) and the upper extremity of 2 bones of the forearm (the olecranon and the radial head). It is maintained by muscles (active stabilizers: biceps, triceps, anconé and extensors and flexors of the wrist) and by ligaments (passive stabilizers: lateral external, internal, anterior, posterior and annular ligaments, radial collateral medial ligaments and articular capsule).
In France, there are less than 1,500 elbow prostheses implanted per year (either partial prostheses with a radial head in the case of fractures or total prostheses of the elbow, for different reasons according to the case). The 3 main clinical situations are: inflammatory arthritis (rheumatoid polyarthritis), osteoarthritis (primary or secondary) and fractures (fracture of the lower extremity of the humerus, the upper extremity of the ulna or the radius).
The clinical signs and symptoms in these different pathologies are pain and stiffness for arthritis and osteoarthritis and for those conditions associated with hematomas, deformations of the elbow with functional incapacity after falls on the wrist (resulting in radial head fractures) or on the elbow with high energy impact in young patients (with a trans-olecranian fracture) or in the elderly (with sus and intercondylian region fractures of the elbow).
Diagnosis:
The clinical examination:
This exam is essential. With the exception of a traumatized elbow, the exam unfolds as follows:
We test the range of motion of the elbow in all areas (flexed, extended, and prosupined), we measure the strength of the extension and the flexion with a dynamometer and the gripping strength of the wrist by grasping if possible. We look for a cracking, kink, rebounding, localized pain with a hematoma indicating traumatic origin. We look at the axis between the humerus and the forearm for deformations. The association with a compressed median nerve of the wrist or ulnar nerve of the elbow should not be overlooked as these can simulate or be related to previous pathologies (paresthesias and percussive irritable neurological syndromes).
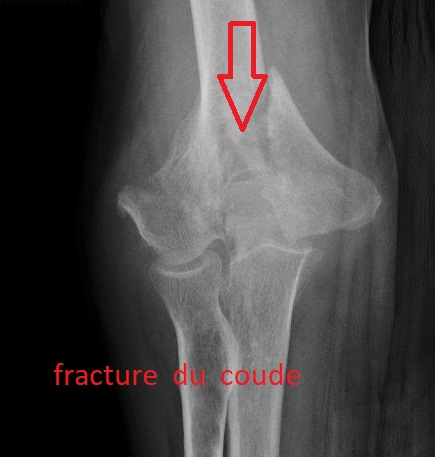
Radiological exams (standard x-rays) allow for the visualization of lesions. These can show bone disintegration in cases of advanced inflammatory arthritis (using Larsen’s classification), the disappearance of the space between the joints with osteophytosis (osteoarthritis), fractures in the humeral plate or of the radial head (Masson’s classification)…
An arthrogram and, possibily, an MRI will be used to establish a record of fractures, evidence inflammatory lesions, tumors and/or in order to plan for the elbow prosthesis.
Before surgery, a dental check-up, ENT and urine laboratory analysis are required to guard against any infections needing treatment beforehand to avoid, by all means possible, any infection of the prosthesis.
An electromyogram will be performed including a speed study in order to seek out any median nerve compression or incidence of ulnar nerve compression, if necessary.
Treatment:
1) For fractures:
If osteosynthesis is impossible, we will propose arthroplasty of the radial head or total arthroplasty of the elbow if the fracture is complex and covers the better part of the articular surface.
2) For arthritis and osteoarthritis:
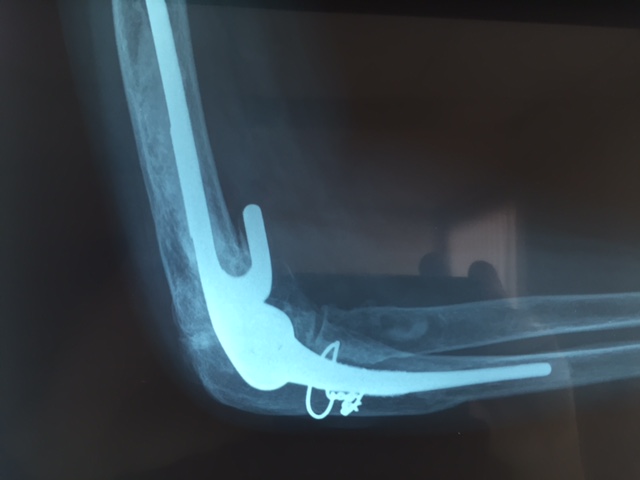
After the failure of a course of medical treatment that has been conscientiously pursued, we will likely propose a partial arthroplasty (radial head) or total arthroplasty (Conrad Moorey’s Prothesis).
Elbow replacement is most often performed under local or general anesthesia, with the patient lying on his/her side, elbow flexed and resting on a half-moon-shaped support at the tourniquet level for total arthroplasties. For prostheses of the radial head, there are two approaches: Cadenat’s posterior approach (by way of the anconeus) and the external approach with patient on his back and arm on the table.
Hospitalization & Recovery:
Hospitalization is usually short. Fingers are immediately mobile since the elbow is immobilized in a sling. Tingling and a loss of sensitivity in the fingers is frequent and recuperation of feeling usually progresses over 3 months to a year only if there is a compression of the median nerve at the wrist or the ulnar nerve on the elbow. Occasionally, as per observation and experience, there can be a transitional period with a hypersensitive reaction.
Complications:
The most frequent:
There is a risk of hematoma, which generally reabsorbs on its own. In exceptional cases, an evacuating puncture or surgical drain might be necessary. Algodystrophy is a painful inflammatory phenomenon, which is not yet well understood. If it occurs, it is treated medically over several months (sometimes over a period of years) and requires specifically adapted rehabilitation, complementary examinations and sometimes specific treatment and care.
The worsening of a compressive syndrome (of the median nerve or the ulnar nerve) can occur that mimicks algoneurodystrophy.
Most rarely:
Deep infection (in the case of arthritis, for example) is possible. It may require additional surgery and extended treatment with antibiotics. It is highly recommended that the patient not smoke or consume unhealthy substances during the healing and scar-formation as tobacco, in particular, increases the risk of infection.
Damage of the radial nerve of the elbow or the ulnar nerve, sometimes the median nerve, that are negatively affected within the fibrous scar tissue or, in highly exceptional cases, sectioned.
The scar can remain swollen and sensitive for several weeks following surgery and sensitive to touch and pressure. Temporary stiffness of the elbow has been observed but usually does not warrant any additional rehabilitation.
Constriction of the carpal tunnel and/or the ulnar nerve of the elbow is possible and can provoke different types of pain that can resemble algodystrophy.
Other complications: stiffness, compartment syndrome, osteosynthetic failure, phlebitis, pyoderma gangrenosum….
Keywords:
Osteochondritis- osteoarthritis of the elbow – rheumatoid synovitis – villonodular synovitis - osteochondromatosis – joint stiffness – radial head fracture – septic arthritis – elbow prothesis – elbow fracture
HAS - Elbow Joint Implants-HAS








elbow and shoulder

elbow

wrist

hip and knee

ankle
![]()
![]()
