






procedure / wrist Carpal tunnel, syndrome of medial nerve compression in the carpal tunnel
Carpal tunnel, syndrome of medial nerve compression in the carpal tunnel

Anatomy:
The median nerve starts in the axillary hole and provides motor function in the forearm and hand and sensory function in the lateral part of the palm of the hand and fingers.
Description and Symptoms:
If there is a compression of the median nerve on the carpal tunnel level in its passage under the anterior annular ligament, this leads to numbness and tingling (paresthesias) in the fingers, most often felt in the first four fingers with the sensation of ankylosis (numbness of the fingers or a heavy arm, sometimes the hypersensitivity felt in fingers is such that one cannot tolerate being touched). At first, these sensations can occur at night then usually occur during effort or use or become constant (variable pains ranging from exacerbated to painless). There can be pain in the fingers or wrist (cracking wrist or fingers) or pain in the fingers and the elbow as well as pain in the wrist or elbow.
Other types of more unusual pains can occur which indicate carpal tunnel syndrome: the feeling of swelling in the arm or fingers, pain in the cervical spinal area (trapezoid cervicalgia simulating cervicobanchial neuralgia), pain in the front of the shoulder (mimicking sub acromial conflict), supraclavicular pain (simulating either first rib syndrome, costoclavicular syndrome or scalene) or breast pain. It can also be associated with burning sensation in the fingers or feeling cold (and the need to wear a glove). Finally, the reasons given for seeing a physician can be isolated or associated to a cyst in the wrist, on the finger or an itchy palm (with eczema lesions), trembling (see the video on youtube in French "tremblement du poignet et de la main"), De Quervain’s tendinitis, arthritis in the fingers (painful fingers, osteoarthritis in the thumb, rizarthritis), Raynaud’s disease…
The wrist might be stiff or blocked (in particular after ligament suturing or a prosthesis operation) or the shoulder might be (capsulite shoulder, see Crymble’s article), motor signs such as dropping objects, losing hand strength, difficulty with fine motor skills (sewing or tweezing). The end result can be a total loss of feeling with amyotrophy of the hand muscles (thenarian). Diabetes, thyroid conditions, rheumatoid arthritis…all favor this syndrome
Diagnosis:
Clinical exams allow for confirmation of this diagnosis. For example: Phalen’s test (provoking pain by bending the wrist forward for an extended period of time, Tinel’s sign (detection of an irritated median nerve at the wrist: eliciting electrical signals by percussing the median nerve at the edge of the carpal tunnel); using the Weber test to check for hypoaesthesia or touching compressed fingers, thenarian amyotrophy (muscle loss at the base of the thumb). Clinical examination can also reveal a compression associated with the ulnar nerve at the elbow. It is also important to verify the absence of “trigger finger”, a finger that locks and suddenly springs up (cracking upon pressure on the palm side of the finger).
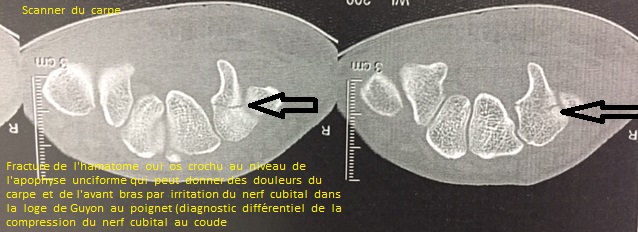
Radiography includes wrist and hand x-rays (frontal and profile views) to seek out any associated bony lesions as well as an electromyogram (40% false negatives: normal EMG) to attempt to confirm the diagnosis of carpal tunnel syndrome. This last exam will determine the degree of severity (conduction blockage) by verifying that the median nerve is not compressed in any other places. It is also important to determine, as is often the case, any compression of the ulnar nerve.
In order to orient the diagnosis, an ultrasound is sometimes indicated (increase in the size of the median nerve at the carpal tunnel) or an MRI of the wrist (swollen appearance of the nerve). The diagnosis is mainly clinical, even in cases of negative complementary tests (infilitration test of corticoids in the carpal tunnel). The patient may be frustrated and discouraged when these exams turn out to be negative.
Treatment:
In the absence of treatment, nerves can lose function. Corticosteroid (cortisone) infiltrations and rest (wrist sling) are the first line of treatment.
In the event that medical treatment fails or severe compression is observed (the collapse of speeds registered on the EMG, anesthesia of the fingers or amyotrophy), surgery will be suggested.
Surgical intervention is most often done under general or local anesthesia.
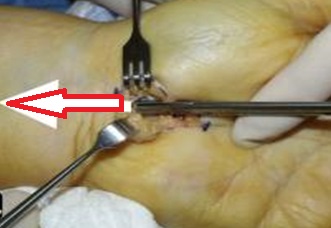
First, the surgeon makes a longitudinal incision in the axis on the radial side of the 4th finger (minimally invasive path of 1.5cm). The anterior annular ligament is opened at the base of the compressed nerve, generally with a simple sectioning of the ligament. A tenosynovectomy may be necessary as well.
Hospitalization & Recovery:
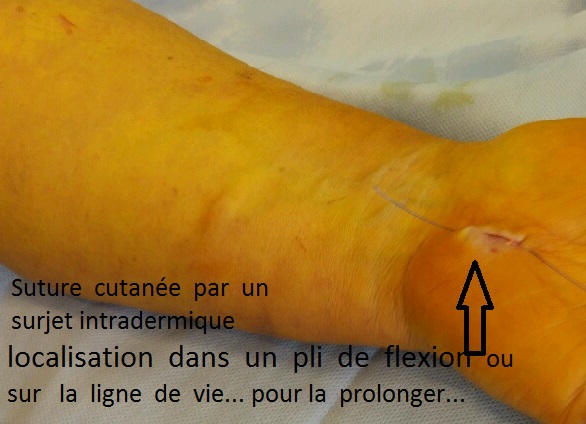
Hospitalization is ambulatory. Fingers and wrist are immediately mobile after surgery. Healing and scarring take from 10 to 15 days
Liberating the median nerve means that pain subsides, sometimes with the immediate disappearance of dyesthesias (except in severe forms) and most often allows for complete recovery in a few weeks.
Partial loss of sensation or motor strength can be observed, often in the event of very serious compression. The results are usually excellent, complications are rare. Strength may be limited for several months. The degree of recovery is unpredictable. Relapse is rare.
Complications:
Hematoma: as with all surgery, there is a risk of hematomas that are generally absorbed on their own. On exceptional occasions, evacuating puncture or surgical drainage is necessary.
Algodystrophy (otherwise known as Complex Regional Pain Syndrome (CRPS) and Reflex Sympathetic Dystrophy Syndrome) is a painful, inflammatory phenomenon that is still not well understood. It is treated medically and can last for several months (even years), requiring specific care with adapted rehabilitation, complementary testing and sometimes pain management. It is unpredictable in its appearance, its evolution and its potential consequences.
Relapse is possible if there is neuropathy (deep anomaly of the nerve).
Deep infection is possible. It may require additional surgery and extended treatment with antibiotics. It is highly recommended not to smoke or consume unhealthy substances during the healing period as tobacco significantly increases the risk of infection.
Neurological incidence on the median nerve (in the fibrous scar tissue or a section of it) is exceptional (partial section or at the thenaraian branch).
Scars can remain swollen and sensitive to touch for several weeks.
Temporary stiffness of the wrist and fingers can be observed and warrants additional rehabilition and physical therapy.
SEE:
KEYWORDS:
Paresthesias - Tinel - Phalen’s Test –Weber’s Test – Cervicobranchial neuralgia – Subacromial – Front shoulder pain – Elbow and wrist pain - Itchiness – Nerve compression of the ulnar nerve – Carpal tunnel – Thenarian Amyotrophy – Finger arthritis – Corticosteroid infiltrations – Raynaud’s syndrome – Stiffness of the wrist or blockage of the wrist - rizarthritis – Burning sensation in the fingers – Finger numbness - Algodystrophy - Fibromyalgia








elbow and shoulder

elbow

wrist

hip and knee

ankle
![]()
![]()
